Depending on which side of the Vindhyas you reside, pain and stiffness in the neck, upper back and shoulder, associated with giddiness or pain shooting down the arms, is almost invariably labelled as either “Cervical” or “Spondylitis,” by laypersons and medical professionals alike. While “Cervical” means neck, the term “Spondylitis” is almost always misused in India since it implies infection (such as tuberculosis) or inflammation (such as Ankylosing Spondylitis or “Bamboo” Spine), both extremely serious conditions.
The term Spondylosis (which is the correct term) refers to degenerative changes (a “wear and tear” phenomenon) noted on x-rays and MRI scans in the discs – the shock absorbers that separate the vertebrae of the spinal column and the facet joints. Some medical practitioners describe this normal ageing process rather ineloquently as a “gap” in the spine.
The typical symptoms of Cervical Spondylosis are a dull ache or stiffness in the neck, sometimes associated with radiating pain down the arms or shoulder blades. The pain is rarely severe, and if described as such or if significant consumption of painkillers is required, other diagnoses must be considered, especially in IT Professionals. Cervical Spondylosis causes a significant problem only when there is pinching of the nerves by a large herniated disc or compression of the spinal cord or vertebral artery by the worn-out vertebrae. Although neck pain is an extremely common symptom, affecting 15% of males and 22% of females, Cervical Spondylosis is rarely the main culprit. This is because, after age 30, the human spine practically always shows changes of degeneration. Numerous studies have been done where people were randomly picked for x-rays or MRI scans. Degenerative changes or disc bulges in the cervical spine were seen in up to 40% of the adult population, and its frequency reached 90% by age 60. Yet most of these subjects were not in pain! Autopsy studies have shown degenerative changes in 60% of females and 80% of males by 49 years.
Degenerative changes in the cervical spine are so prevalent that the mere presence of such abnormalities cannot be taken as prima facie evidence of the causality of pain. If you took a random sample of middle-aged workers in any of our offices and performed screening x-rays or MRI scans, the majority would have reportable “abnormalities”. If you are an adult and, based on a spine x-ray, CT or MRI scan, have been reported as having “spondylitis” or a disc bulge, you are probably normal for your age. Your x-ray or MRI may be suffering from “spondylitis”, but the true source of your pain may lie elsewhere!
What is it, then?
Welcome to the world of Repetitive Strain Injury, or RSI!
RSI refers to a constellation of work-related overuse disorders due to diffuse involvement of muscle, fascia (connective tissue covering muscles), tendon and/or neurovascular structures, typically involving the neck and upper limb. However, any part of the body, e.g., the back, legs, eyes, vocal cords, etc., may be affected. RSI is known in medical circles as Work Related Musculoskeletal Disorder (WRMSD) since repetitive activity is not the sole nor the main factor causing these disorders.
Arising as aches and pains or numbness, these injuries can progress to become crippling disorders that prevent sufferers from working or leading normal lives. RSI is usually the consequence of neglecting Ergonomics and is India’s number one Occupational Health concern.
The world’s largest study on RSI covering over 35,000 Indian IT professionals (2011), conducted by RECOUP, Bangalore, reported that over 75% reported musculoskeletal symptoms related to work and 55% got injured within a year of starting their first job. Over 1000 young IT/ITES Professionals have lost their livelihood because of advanced, neglected RSI resulting in Type 1 Complex Regional Pain Syndrome. In the past 2 decades, RECOUP has treated over 10,00,000 RSI patients from 45 countries, of which nearly 40% were musicians, laboratory staff, bankers, teachers, journalists, RJ’s, dentists, nurses, surgeons, physiotherapists, children and housewives and the remaining 60% were office professionals working on computers.
The commonest areas affected include the neck and upper back (60%), followed by the lower back (40%) and the upper extremity (30%). In 20%, it was a generalised disorder associated with constant pain and numbness. The commonest types of RSI seen are Myofascial Pain Syndrome (due to an exquisitely sensitive knot within the muscle belly), Thoracic Outlet Syndrome (compression of the nerves and blood vessels between the base of the neck and armpit) and Cubital Tunnel Syndrome (compression and tethering of ulnar nerve at elbow). All three can cause “referred pain” or sensations at a point away from the actual trouble spot. Together, Thoracic Outlet Syndrome and Myofascial Pain Syndrome account for over 95% of RSI cases in India.
According to RECOUP’s study, the commonest risk factors for RSI were lack of appropriate breaks and poor office ergonomics. Other common causes include intense, repetitive work, static postures, mental stress at work/home, anxiety, depression and job dissatisfaction. Over 60% of individuals diagnosed to have RSI had received no training in Ergonomics at their offices, and another 30% had received incorrect ergonomic advice from furniture vendors or doctors/physiotherapists with inadequate knowledge or qualifications in Ergonomics.
Common Symptoms of RSI
The symptoms are:
- Discomfort, fatigue or pain (sudden or gradual)
- Swelling, redness, paleness or warmth
- “Catching” (pinching sensation) or “snapping” (crepitus) associated with movement
- Loss of grip strength (muscle weakness), heaviness or clumsiness of the hand
- Decreased range of motion or stiffness
- Burning, numbness, tingling, “pins and needles”
- A constant need to stretch or massage one’s arms
- Visual strain or fatigue while working
- The slow accumulation of injury occurs with a gradual development of difficulty in day-to-day activities such as shaking hands, opening doors, holding newspapers, using a comb, or even holding a teacup
When you develop these symptoms, DO NOT
- Start using the left hand for the mouse
- Take a vacation, hoping the pain will go away with rest. Not only will the pain return when you get back to work, but you could also be left without adequate medical leave!
- Self-medicate (painkillers, ointments, alternative medicine)
- Use a neck collar, lumbar brace, crepe bandage or wrist splint (especially while working)
- Join a gym or start weight training
- Start swimming
- Undergo vigorous oil massage, manipulation or chiropractic
- Start isometric/resistive neck exercise
- Take absolute bed rest beyond 1-2 days to avoid stiffness, muscle wasting, loss of bone mineral density, and chronic disability. Stay as active as possible and return early to normal activities, including work.
- Sleep on the floor and stop using a pillow. Use a firm mattress and a thin, firm pillow that supports the head, neck and upper back.
- Undergo passive treatment modalities (massage, ultrasound, electrotherapy, or traction)
All these modalities have the potential to worsen your existing situation.
When should you seek medical help?
The potential for full recovery is enhanced if individuals seek competent medical help for early symptoms. It is now known that most cases of severe RSI start with vague discomfort in the neck and shoulders, which, if neglected, lead to incapacitating pain, burning or weakness in the hands, precluding usage of the hands. As a general rule, seek expert care AS SOON AS POSSIBLE because a delay of a few days could make the difference between a quick and complete recovery and a long-drawn struggle to overcome RSI. It is worth seeking references from injured co-workers or friends before choosing your doctor, rather than trying out the nearest Physician, Orthopaedist, Neurosurgeon, Physiotherapist or Corporate Hospital that you can find. Remember: choosing medical professionals to treat your RSI is the most critical factor towards your recovery. Seek a Rehabilitation Physician with a proven track record in diagnosing and treating RSIs sooner rather than as a last resort. The Physician must lead an interdisciplinary team comprising lifestyle and functional medicine physicians, occupational health physicians, ergonomists, physiotherapists, aquatic therapists, biofeedback therapists, clinical psychologists, nutritionists, specialist pain health coaches (care captains), etc.
Computer users typically underestimate the seriousness of RSI, and many are unaware that it can lead to job losses. On developing symptoms, many individuals waste precious time trying home remedies or procrastinating (But I have always been fit and healthy…Could it be RSI? Is it an Ortho problem or a Neuro problem? Why are my co-workers not in pain? But I type only for a few hours…). Many waste crucial time in support groups and online forums trying to get a cure from laypersons or quacks.
Many Indian IT Professionals are reluctant to admit having RSI for fear of retrenchment and feel uncomfortable or embarrassed asking for ergonomic modifications to their workstations, unsure of their managers’ support. They seek medical help usually at a stage when they cannot work any longer and come begging for confidentiality. Many do not seek medical help because of fear of being labelled “sissy”, “psychotic”, or an “incurable” and hence “unemployable” RSI victim. Another popular misconception is that since muscle pain is “incurable,” there is no point in complaining about it.
RSI is a progressive and cumulative disorder, which, if neglected, could lead to permanent structural damage, leading to an inability to work or to lead a normal life.
What are the solutions for RSI?
Studies have shown that employees who turn up to work despite pain (presenteeism) cause massive productivity losses to their employers.
All organisations, big and small, must invest in comprehensive Ergonomic Intervention Programmes with both proactive (mandatory training on Ergonomics, Posture, Individual Workstation Assessments and Fitness sessions) and reactive (early on-site RSI therapy and Workplace accommodation procedures for injured workers) elements. A study published in 2019 on the effectiveness of this treatment protocol in managing WRMSD in 12000 IT professionals (doi: 10.1007/978-3-319-96080-7_77) found that 94% of workers reported complete resolution of symptoms and 6% reported partial resolution of symptoms but could work without restriction.
No employee had to take leave for more than 7 days or leave the job due to WRMSD.
Remote RSI Intervention (2020-2023) in 5000+ IT Professionals, comprising Occupational health teleconsultation, Telerehabilitation, including exercises, self-help remedies, Functional/Lifestyle medicine interventions; Psychological/behavioural approaches, and Virtual ergonomic workplace analysis reported that 92% of workers reported either complete or near-complete resolution of symptoms, and 8% reported a partial recovery. 96% reported a significant improvement in work productivity and quality of life. No worker had to stop working due to WRMSD.
Worker productivity increased by 20%, and the company saved Rs. 25,000 per worker per annum because of RECOUP’s Ergonomics Intervention Programme (doi: 10.3233/WOR-2012-1048-5921).
The benefits of the comprehensive approach, according to the study, included healthier employees, increased productivity, fewer errors, increased competitiveness in the marketplace, less absenteeism, increased job satisfaction and job retention, reduced employee group health insurance costs, and greater goodwill for the employer in the society.
True Case History
Mr. X, a 40-year-old top-ranking executive of one of India’s best-known IT firms based in Bengaluru, had a nagging mid-back discomfort for 6 weeks, which appeared primarily at night and woke him from sleep. He had no known medical illnesses, was an ardent yoga practitioner and had no other significant symptoms. He sequentially consulted a series of physicians, neurosurgeons, and practitioners of ayurveda and homoeopathy, physiotherapy and acupressure. He had a series of normal blood tests, x-rays, and MRI scans which showed minor degenerative changes in the thoracolumbar spine.
Each time he was diagnosed with “spondylitis” and “stress” and treated with painkillers, antidepressants and a wide variety of alternative medicine and physical therapies, without relief. When he finally consulted me, I found no physical evidence of pain originating from the musculoskeletal system. I immediately ordered a spiral CT scan of the abdomen and, within hours, found my worst suspicion come true: Non-Hodgkin Lymphoma in the retroperitoneal region – nasty cancer! In my over 12 years of medical practice in Bengaluru, I have unfortunately seen this story repeat with minor variations several times.
So, what are the lessons to be learnt from this sorry episode?
- IT professionals try to obtain a quick fix by somehow controlling pain to allow a quick return to work.
- Every possible type of alternative therapy is fair game in India, and IT Professionals ignore scientific rationale. Most practitioners anoint themselves “doctors” and work under no significant regulation and the reassurance that the authorities are more than willing to turn a blind eye to the consequences of therapeutic misadventures under the guise of these therapies supposedly being time tested, traditional, devoid of side effects or cheap.
- Self-diagnosis, internet-based diagnosis and an assumption that the treatment of back pain is physiotherapy or yoga could be life-threatening.
What is the current scenario in India?
- Early identification of RSI and competent medical intervention are critical to arresting and reversing the injury in its early stages.
- Unfortunately, Indian medical professionals (in general) are not equipped to diagnose or treat RSIs since it is a relatively recent phenomenon in our country, and no training courses for doctors exist. Ergonomics, RSI and Myofascial Pain Syndrome do not even find a passing mention in the Indian Medical Curriculum. It is not unusual to find Indian doctors (even specialists) and physiotherapists who have not even heard of RSI.
Pitfalls in the treatment of RSI
- Misdiagnosis as “Spondylitis”, “Arthritis” (Tuberculosis and gout being the popular ones!), ‘Slipped Disc”, “Muscle Sprain” or “Carpal Tunnel Syndrome” seems to be the rule rather than an exception. Diagnosis of RSI is entirely based on a skilled musculoskeletal examination by an expert, and no “special” tests including MRI scans or nerve conduction studies can reliably diagnose it.
- Inappropriate medications, e.g., corticosteroids (or Cortisone), antidepressants, Vitamin injections, Unspecified “Health Pills”, etc. Medicines and potions (Allopathic or Alternative) make little difference in the long term.
- Conventional physiotherapy is usually ineffective (Ultrasound, Short Wave Diathermy, etc.) and sometimes dangerous (traction and isometric/resistive neck exercises).
- Inappropriate surgery for a presumed diagnosis of Carpal Tunnel Syndrome or Slipped Disc, with disastrous consequences.
- Total reliance on fancy ergonomic gadgetry, special chairs, wrist rests, split keyboards, anti-glare screens, etc., to prevent RSI while ignoring human factors (e.g., practical training in posture, body awareness, typing technique, breaks).
- Often, RSI sufferers are told, “it’s all in your mind”, and the only way to treat it is to get “it out of your mind”! No further clues are usually provided on how to achieve this laudable goal. Worse, others are condemned to referral to a psychiatrist because the “specialist” could not find anything wrong on examination or investigations.
- No significant attempts at identifying and correcting predisposing factors for RSI, e.g., ergonomic or postural problems, medical comorbidities, habitual deep muscle tension, etc.
- Alternative medicine practitioners who practice a single technique often have a single-track approach to diagnosis and treatment (“when the only tool you have is a hammer, everything looks like a nail!”). Most have no knowledge of RSI, which can severely aggravate an existing RSI and prolong recovery. However, some modalities like Yoga, when used appropriately and in a holistic, interdisciplinary environment, are beneficial in RSI.
On the lookout for a quick fix requiring minimum effort and time off work, RSI victims usually run from pillar to post seeking effective treatment and often fall victim to quacks. The gullible computer users swallow up inaccurate and unmoderated information abundantly available on the Internet, adding to their plight.
No two patients with RSI or chronic pain have the same condition and are unlikely to respond to the same treatment. Successful recovery requires precision medicine based on individual phenotype and endotype and systematic, personalised, comprehensive biopsychosocial rehabilitation based on epigenetic, occupational, and lifestyle risk factors and addressing comorbidities. This approach has enabled over 10,00,000 patients from 45 countries to reclaim their lives and careers. Some patients have remained pain-free for over 20 years despite being disabled due to intractable and agonising pain for months or years.
Appropriate treatment for RSI
- The assessment includes a comprehensive musculoskeletal/myofascial examination focusing on the range of motion, trigger points, biomechanical problems, and evidence of nerve or blood vessel entrapment, plus any other pertinent tests according to the presenting symptoms. Further assessments may include a workstation evaluation focusing on biomechanical and ergonomic issues, nerve conduction studies, x-rays, MRI and occasionally, psychological assessment. After the assessment, an individualised treatment plan is proposed.
- We have developed our treatment method for RSI called the SHARAN’S Protocol (Skilled Hands-on Approach for Release of myofascia, Articular, Neural and Soft-tissue mobilisation). Before starting treatment, I make a specific diagnosis and outline the treatment goals for our rehabilitation team. I supervise the treatment and review patients at least once a week, occasionally modifying treatment or stopping for further investigations if necessary. In phase 1, when the patient has severe discomfort, we use combinations of modalities like ischaemic compression, deep-pressure soft tissue massage, myofascial release, voluntary contraction and release methods, muscle energy techniques, positional release techniques, relaxation techniques, breathing exercises, Kinesio taping, Interferential Therapy (IFT), Ultrasound, Laser, spray and stretch and needling (TrP injections). In phase 2, when the patient has moderate discomfort, we use manual techniques to increase the flexibility of affected tissues by soft tissue, neural, and articular (rib / clavicular/scapulothoracic/spinal) mobilisation. Patients initiate self-stretching exercises, nerve and tendon glides, and start body awareness techniques like the Alexander technique and Yoga. In phase 3 (mild discomfort), the emphasis is on further self-stretching exercises, progressive strengthening exercises, postural retraining, body mechanics and ergonomics training on a model computer workstation, ergonomic furniture and accessory recommendation, and gradually preparing patients to return to work. In phase 4 (maintenance phase), there is further strength training, aerobic conditioning, Yoga and Tai Chi.
- The treatment also includes adequate education to allow individuals to adopt healthy work habits and exercises for maintenance. The treatment of RSI requires that individuals take responsibility for changing their approach to work and other activities. The most challenging part of the treatment is to tackle “habitual deep muscle tension” in the neck and upper back that happens each time the person sits in front of the computer because medical professionals are not usually around to identify it or address it when it happens. We have had the greatest success with body awareness techniques like the Alexander technique, Yoga, Feldenkrais and EMG Biofeedback for this. Training with wearable surface EMG Biofeedback to reduce muscle tension; with a wearable Neurofeedback device for stress and insomnia; Personal wearable posture monitor/sensor; Somatic biofeedback using a pulse oximeter, heart rate variability, thermography, plethysmography and activity monitors; with Intelligent Device for Energy Expenditure and Activity (The IDEEA® system).
- We do not recommend using a cervical collar, lumbar braces or wrist splints, especially while working. Simply taking rest rarely helps, and the pain usually returns on the first day back at work. Surgery is seldom indicated. Common co-existing conditions like hyperuricemia, anaemia and micronutrient deficiencies, hypothyroidism, osteoporosis and inflammatory arthritis require medical treatment.
- In most cases, except the mild ones, self-treatment can achieve only so much, and people then have to reconcile to “managing” RSI throughout their lives. Expert hands-on RSI treatment at the correct time is the most crucial determinant of complete recovery. Another thing that needs to be told is that RSI is usually relentlessly progressive, and some untreated cases or poorly treated cases end up with a dreaded complication called Type 1 Complex Regional Pain Syndrome, after which patients lose the use of their hands. Forget typing; we have had patients unable to perform simple activities like eating, bathing, dressing, opening door knobs or holding a teacup. All these people ignored early symptoms thinking nothing serious could happen to them or had been self-treating them. According to our published research, the average time it takes for localised RSI to become generalised or complicated is 6 months.
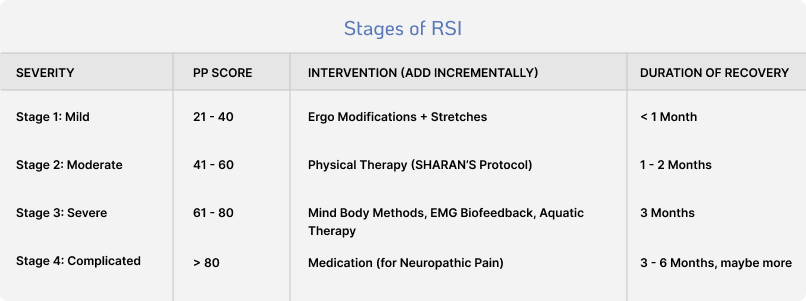
DEEPAK SHARAN’S Pain Phenotype Score
Disability beliefs
Effect on daily activities
Effect on self-efficacy
Pain intensity and nature
Ability to work
Known mental distress
Sensitisation
Hours of continuous pain per day
Area affected (out of – neck, shoulder, elbow, wrist/hand, upper back, lower back, hip/thigh/buttock, knee, ankle/feet)
Recovery expectations
Avoidance behaviour
Nerve-related symptoms
Sleep disturbance
Perceived injustice
Pain catastrophising
Self-perception
People commonly ask why, when so many people are doing identical work, some people get injured, not others.The answer lies in differences in knowledge of safe computing techniques, anatomy (body flexibility, upper body strength, etc.), workstyle, ability to pace one’s work, and the ability to manage stress.
Workstyle refers to a “behavioural, cognitive and physiological response that can occur in individuals due to increased work demands.” In a large study on 4500 IT professionals, 22% reported having an adverse workstyle, and 63% reported pain symptoms. Social reactivity, lack of breaks, and deadlines/pressure were significantly correlated with pain and loss of productivity (Sharan D et al., 2011).
Tips for prevention
Reduce stress:
- Take a 5-second typing break (“micro-break”) every 5-7 minutes and at least a 2-minute break every 30-40 minutes (“macro-break”). Get a timer and set it for 30-minute intervals or use Break-Reminder Software. Don’t let this stretch to more than an hour.Get up, walk around, stretch your back, and swing your arms.Have a glass of water or visit the loo.Talk with someone about topics unrelated to work. Give your mind and body a rest.
- Learn correct typing techniques, balanced computing posture, equipment setup, and good work habits.
- Hold the mouse lightly and use 2 fingers for clicking. Get your hands away from the mouse when you are not using it.
- Keep your arms and hands warm.
- Massage your hands and forearms several times daily with vitamin E lotion. The massage will improve circulation and break up adhesions. Since you can’t touch a keyboard until the lotion is absorbed, it also enforces a good break.
- Massage the muscles in your neck, working your way down from the skull to the shoulders, applying more force to the larger muscles as you go down.
- Periodically evaluate your environment for ways to reduce stress. Try to keep your desk uncluttered so you can always find things. Ensure programmes are set up correctly on the computer, and see if you can use a macro program to reduce keystrokes.
- Drink plenty of water (6-8 glasses) during the day. Juice and soda are not substitutes for pure water.
- If telephone use is frequent, use a headset instead of a handset.
- Emphasise diaphragmatic (abdominal) breathing to reduce pressure on your chest.
- When faced with unavoidable stress, step back and evaluate your reactions. You can’t eliminate stress in life, but you can modify your reactions, so they don’t harm you.
Workstation and posture checklist:
- Neutral position means sitting up, head straight, with eyes looking forward
- Sit centred in front of the monitor
- Tailor your workplace for your height.The top of the monitor should be at eye level.Eyes look down at the monitor at a 15-20 degree angle.
- When typing from reports, etc., use paper holders (metal and plastic) to keep papers at eye level.
- Sit with feet flat on the floor, some weight on the feet
- Hips slightly higher than knees
- Neutral spine and neck posture
- Do not crane your head and shoulders forward to look at the computer screen: your neck isn’t designed to hold the weight.
- Shoulders down and back
- Chin tuck
- Elbows held loosely against the sides of the chest
- Wrists slightly lower than elbows
- Wrists straight or slightly drooped. Palms parallel to the keyboard
- Forearm horizontal
- Relaxed, curved fingers
- Type with the tip of your fingers
- Do not rest any body part on wrist rests or the edge of the desk or keyboard tray when typing.
- While typing or mousing, the keyboard is lowered and angled slightly away from you (negative pitch or tilt).
- Frequent changes in the position of the hands, arms, and trunk
Tips to prevent visual strain:
- Looking at the monitor for extended periods can cause eyestrain. Eyestrain means different things to different people. Depending on the person, it may be experienced as burning, tightness, sharp pains, dull pains, watering, blurring, double vision, headaches, and other sensations.
- The major factors affecting the eye of a computer user are glare, luminance, the distance between eye and screen, readability of the screen and document, the user’s vision and his/her corrective lenses.
- Keep the monitor as far away as you can read comfortably from your neutral sitting position. The top of the screen should be just below eye height.
- Proper lighting for your work area is important. While you want to be sure you can see your work, you also want to avoid looking directly at a light source or having glare reflected off your screen.
- Lighting should be indirect and even. Don’t aim a light at your reference documents; be sure you’re not facing a light or a window.
- Place your monitor at a 90-degree angle to windows and other direct sources of light. A tiltable monitor stand will enable you to adjust to different lights.
- Keep your monitor screen clean. Wipe it with a slightly wet, lint-free cloth every day before you start work.
- Set the brightness of your monitor at about the same level as that of objects in your field of vision, such as the wall in front of you. And keep reference documents at about the same distance away from you as the screen. For comfortable viewing
- The brightness and contrast control of the monitor should be set properly for comfortable viewing. Turn the brightness to a minimum, then set the contrast to a level comfortable for your viewing.
- The natural mechanism of blinking gives our eyes micro rest. When people view the computer monitor, their eye-blinking rate goes down drastically. With little effort, this can be corrected. For a few days, consciously try to blink at the normal rate. If practised for a week or two, you can regain your natural blinking rate when using the computer. This can reduce eye strain to a good extent.
- Rest your eyes by periodically focusing on distant and near objects quickly. Reduced eye fatigue reduces stress.
- Exercise your eye muscles by tracing an X in a box; look as far to the sides as possible.
Seating:
A well-designed chair will favourably affect posture, circulation and the amount of strain on the spine. The preferred way of sitting involves the following:
- Make sure that the seat height is correctly adjusted so that your feet are on the ground or on a solid surface like a good footrest.
- Recline back in the chair, with the chair backrest angled between 100-110-degrees, so that the chair back can help support the weight of the torso.
- Make sure that the chair has good lumbar support in the right area for your shape and size of back. If there is an adjustable support, use this to get the best position. If not, use a rolled towel or a cushion to improve your lower back support.
- Make sure that the seat pan is the right size for you and doesn’t press behind your knees.
- Look for a chair that doesn’t tip up the seat pan when you recline because this can put pressure under the thighs and behind the knees.
- If the chair has arms, ensure that these are correctly adjusted for height so that your shoulders are relaxed, not hunched or raised, when you rest on the armrests.
- If the chair has a high neck/headrest, ensure that this can be used in different sitting positions.
Typing Technique:
- Don’t bend your wrists sideways or upwards
- Let your elbows swing freely
- Keep your fingers in a curve
- Keep your thumbs, 4th and 5th finger relaxed
- Don’t slap the keys – use finger press, not tapping action with hand and wrist
- Try to type with rhythm, using smooth, elegant movements
- No gymnastics!
- Adopt keyboarding techniques that emphasise the use of large muscles, such as the shoulders and upper arms, instead of small muscles, such as those that drive the fingers
Deep Breathing
Deep breathing is the simplest and most effective relaxation technique. Shallow, rapid breathing is a common stress reaction. So deep, slow breathing can interrupt your stress response and help you to relax.
Close your eyes. Breathe out slowly and completely through your mouth. Watch your stomach “cave in” as you breathe out. Now breathe in slowly and deeply through your nose. Watch your stomach expand as you breathe in. Hold for five seconds, then exhale and begin the cycle again. Repeat at least five times.
If work causes pain, it is not normal, and something needs to be done about it.
About Dr Deepak Sharan
- Chairperson, Scientific Committee on Musculoskeletal Disorders, International Commission on
- Occupational Health, 2022-2024
- President, International Myopain Society
- Founder Director, EPM International Ergonomics School, Italy.
- Founder President, Indian Ergonomics School.
- Founder President, Indian Myopain Society
- Over 500 International scientific publications or conference presentations, including some of the world’s largest epidemiological studies in Office and Industrial Ergonomics, Healthcare Ergonomics, Cognitive Ergonomics and Work-Related Musculoskeletal Disorders (WRMSD).
- Co-developed the Time-based Assessment Computerised Strategy (TACOs) to assess the risk of WRMSD among Physiotherapists.
- Winner of several Awards and Research Grants, including the National Disability Award (Government of India) and the World’s highest Research Awards in Orthopaedics and Paediatric Orthopaedics.
- An internationally recognised expert in WRMSD, having developed his validated assessment and treatment approach called the DEEPAK SHARAN’s Pain Phenotype Score and the SHARAN’s Protocol.
- Successfully treated over 10,000,00 patients with WRMSD from 45 countries.
- Ergonomics and Occupational Health Consultant to several Fortune 500 companies.
- Certified Worksite Wellness Specialist (USA) with proven expertise in conducting comprehensive on-site and remote Occupational Health programs incorporating Functional Medicine.
- The only authorised trainer in all English-speaking countries for Revised NIOSH Lifting Equation, ERGOcheck Risk Mapping, TACOs Tool, OCRA methods, and Push-Pull-Carry – gold standard tools for assessing the Ergonomic risk factors involved in biomechanical overload due to repetitive activities and manual material handling according to the current ISO standards for Ergonomics (ISO 11226 and 11228).
- Organising Chairperson, PREMUS: the 11th International Scientific Conference on the Prevention of Work-Related Musculoskeletal Disorders, WDPI: the 6th Work, Disability, Prevention and Integration Conference, and MYOPAIN: the 11th International Conference on Myofascial Pain Syndrome and Fibromyalgia Syndrome, September 20-26, 2023, Bengaluru, India (premus2023.com)